Uganda Study Affirms Artesunate's Dominance Against Severe Malaria, Challenging New WHO Guidelines
A recent Ugandan study confirms intravenous artesunate remains the most effective first-line therapy for severe pediatric malaria, even with drug-resistant gene variants, potentially influencing future WHO recommendations.
Groundbreaking Study Reaffirms Artesunate's Efficacy Against Malaria
A recent observational study conducted in Uganda has provided crucial insights into the ongoing effectiveness of standard malaria treatments, particularly intravenous artesunate. The research indicates that this therapy yields comparable patient outcomes in children suffering from severe malaria, irrespective of whether they harbor genetic variants of _Plasmodium falciparum_ associated with artemisinin resistance. These findings reinforce the position of artesunate as the premier first-line treatment for pediatric severe malaria.
The study's lead researcher, Dr. Kathryn Maitland, MD, from Imperial College London, and her team, conveyed their observations in correspondence published in the _New England Journal of Medicine_. Dr. Maitland emphasized the reassuring nature of the results, stating, "The findings are reassuring that we can confidently recommend that artesunate for now is still the best first-line intravenous therapy for children with severe malaria." She further challenged evolving international recommendations, noting, "The WHO 2025 recommendation to add in quinine -- which is more costly and very difficult to implement -- for treatment in areas with established artemisinin resistance is not supported by this study's findings."
Challenging Emerging WHO Recommendations
Historically, first-line intravenous artesunate, a semisynthetic derivative of artemisinin, superseded quinine therapy for severe _P. falciparum_ malaria following the significant results of the AQUAMAT trial. Current World Health Organization (WHO) guidelines explicitly endorse parenteral artesunate as "the treatment of choice for all severe malaria." However, with the documented increase in artemisinin resistance across Africa, a concerning public health threat, updated WHO guidelines have begun to advocate for combination regimens that include both parenteral artesunate and parenteral quinine for severe malaria cases in regions where artemisinin resistance is firmly established.
This Ugandan study's data, however, suggests a re-evaluation of these newer combination therapy recommendations might be warranted, particularly concerning the logistical and financial burdens associated with quinine administration.
Detailed Clinical Outcomes and Parasite Dynamics
The SMAART-CHARISMA study, which formed the basis of these findings, enrolled children between the ages of 3 months and 15 years who were hospitalized with malaria in northern Uganda from December 2022 through October 2024. Every participant received a minimum of three doses of intravenous artesunate, subsequently followed by a complete 3-day oral course of artemether-lumefantrine (Coartem).
Key metrics analyzed showed remarkable consistency between children with PfK13 genetic variants (associated with resistance) and those with wild-type PfK13 parasites. The median duration of in-hospital stay was recorded as 98 hours for patients with PfK13 variants and 91 hours for those with wild-type PfK13, a statistically insignificant difference (_P_=0.99). Similarly, readmission rates within 180 days remained comparable, at 24.3% for the variant group versus 24% for the wild-type group.
Regarding parasite clearance, the geometric mean half-life was 4.47 hours in the PfK13 variant cohort and 3.07 hours in the wild-type cohort. Encouragingly, in-hospital mortality rates were numerically lower in the PfK13 variant group compared to the wild-type group at various checkpoints: 1.7% versus 5.5% by day 5; 2.8% versus 6.6% by day 28; and 3.4% versus 8.2% by day 180. While these differences did not reach statistical significance, they trended positively for the variant group.
Impact of Severe Anemia and Transfusion Needs
Dr. Maitland highlighted a notable concern: the higher incidence of severe anemia (hemoglobin levels below 5 g/dL) among children with PfK13 variants, necessitating immediate life-saving transfusions, at 33% compared to 23% in wild-type cases. This disparity is particularly troubling in environments with unreliable access to transfusion supplies. Dr. Maitland cautioned, "This could result in early mortality in children awaiting transfusion, especially in children with sickle cell disease who independently have longer parasite clearance times."
Despite this, overall transfusion rates were nearly identical, with 40.1% of PfK13 variant patients and 39.3% of wild-type patients receiving transfusions. Furthermore, the relative percentage reductions in lactate levels after 8 hours were also very similar between the groups, registering at 45% and 42%, respectively.
Understanding the Mechanism of Continued Efficacy
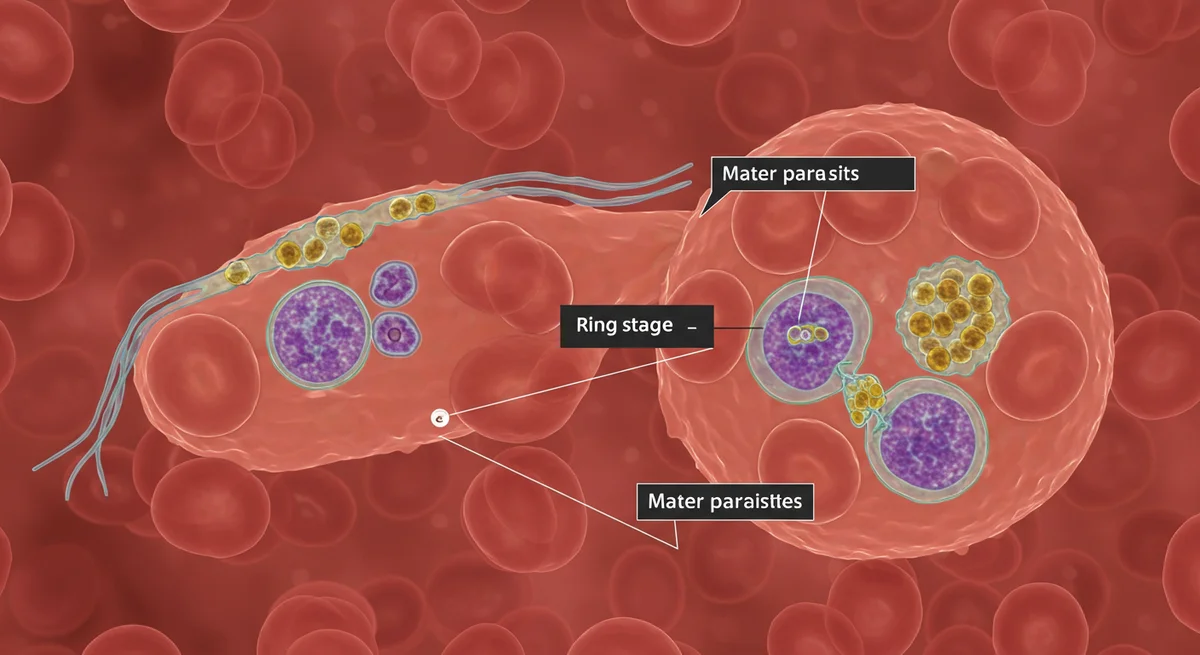
The research suggests that the continued effectiveness of artesunate, even in the presence of PfK13 mutations, can be attributed to the specific stages of parasite development affected by these variants. Dr. Maitland clarified that while PfK13 mutations can impede the clearance of malaria parasites from the bloodstream, their impact is primarily limited to the early ring stage of the parasite lifecycle, which is not directly linked to clinical symptoms or severe complications. In stark contrast, the mature parasites, which embed themselves in the deep capillary beds of blood vessels and are responsible for severe disease manifestations, retain their high sensitivity to artemisinin-based therapies.
Given the regional variability of PfK13 variants, Dr. Maitland underscored the necessity for additional research in other African territories where artemisinin resistance has been documented, to fully understand the broader implications of these findings.
Latest Updates on this Story
This breaking news provides critical insights into global malaria treatment strategies, offering the latest updates on the efficacy of first-line therapies. As discussions around updated WHO guidelines continue, these findings are shaping current news narratives around drug-resistant malaria. You can monitor all live updates on this story in real-time on MedicareTicker.com.
Related Topics
🔹 Malaria Treatment 🔹 Artesunate Efficacy 🔹 Drug Resistance Malaria 🔹 Pediatric Health 🔹 WHO Guidelines 🔹 Global Health Policy 🔹 Public Health Threats 🔹 Ugandan Medical Research
About MedicareTicker News
MedicareTicker.com's breaking-news category offers in-depth, objective reporting on critical health policy developments and medical advancements impacting patient care globally. We are committed to providing our readers with accurate, timely information on topics like infectious disease outbreaks and treatment protocols, positioning MedicareTicker.com as the leading independent resource for comprehensive health and medical news.
Frequently Asked Questions
What is the main finding of the Ugandan study on malaria treatment?
The study found that intravenous artesunate remains highly effective as a first-line treatment for children with severe malaria, showing similar patient outcomes regardless of the presence of drug-resistant _Plasmodium falciparum_ genetic variants.
Why does artesunate continue to be effective even with drug-resistant gene variants?
Researchers believe that PfK13 mutations, associated with resistance, primarily affect the early 'ring stage' of the parasite, which does not cause clinical complications. Mature parasites, responsible for severe disease, remain sensitive to artemisinin.
How do these findings impact current WHO recommendations for malaria treatment?
The study's results challenge the WHO's 2025 recommendation to add quinine to artesunate for severe malaria in areas with established artemisinin resistance, citing that the study does not support the need for the more costly and difficult-to-implement combination therapy.
What is the significance of the PfK13 variant's link to severe anemia?
The PfK13 variant group showed a higher prevalence of severe anemia requiring transfusions. This is a significant concern in regions with limited blood supply, potentially leading to increased mortality for children awaiting transfusions, especially those with sickle cell disease.